
DrCarney.com Blog
Ken's Type-1 Diabetes Journey: Control
My previous doctor(s) informed me that no matter how diligently I controlled my diabetes that I will still suffer diabetic complications. I believe this is said because the conventionally prescribed A1C levels of 6 to 7 percent, for Type-1 diabetics are damagingly high. Further evidence is that my energy levels are lower in the 6 to 7 range as when it is in the normal, non-diabetic 4 to 6 range. In fact the difference in energy / feel-good level is quite profound. With that, my interest was / is to maintain normal – non-diabetic blood-sugars at ALL times (70 mg/dl to 100 mg/dl); not just average or fasting, but always, even after an uncomfortably stuffed high carb meal. And by the way - still no diabetic complications. J
Conventional wisdom for diabetic management is to diligently avoid sugar [carbohydrates]. Everything else goes - just no sugar. Learning diabetic management without conventional wisdom, however, has revealed that sugar is not an issue at all. It is fat and animal products that make sugar an issue. That seems to be a fundamental difference between conventional diabetes management and the management method that I have learned to enjoy.
As mentioned in previous posts, including My Story and Fad Diets Part 2, I discovered the optimum diet by trial-and-error test-and-measure logging. This was, fortunately, due to a lack of otherwise functional information and support. This was equally true regarding blood-sugar control. The result is a rather unconventional control method.
Conventional Type-1 diabetic control is an attempt to mimic the natural biological method where the pancreas senses blood-sugar and secrets insulin into the blood stream in response. The problem with that method is the subcutaneous injected insulin does not track exactly the same as pancreas insulin. Insulin / energy requirements vary from minute to minute – much too fast for injected insulin. To compensate, conventional Type-1 diabetes recommendations call for chronic elevated blood-sugars; A1C numbers between 6 and 7 and blood-sugar levels up to 240 mg/dl. This is for safety reasons; the high numbers provide a buffer to prevent life threatening hypoglycemia (usually referred to as a low). With my control scheme, however, there is no worry about going low; in fact, going low is an intended element of the control method. I know, this sounds crazy, and, no, the intent is not really to end up with low blood-sugar. Instead, it is to only head that way. Please read on…
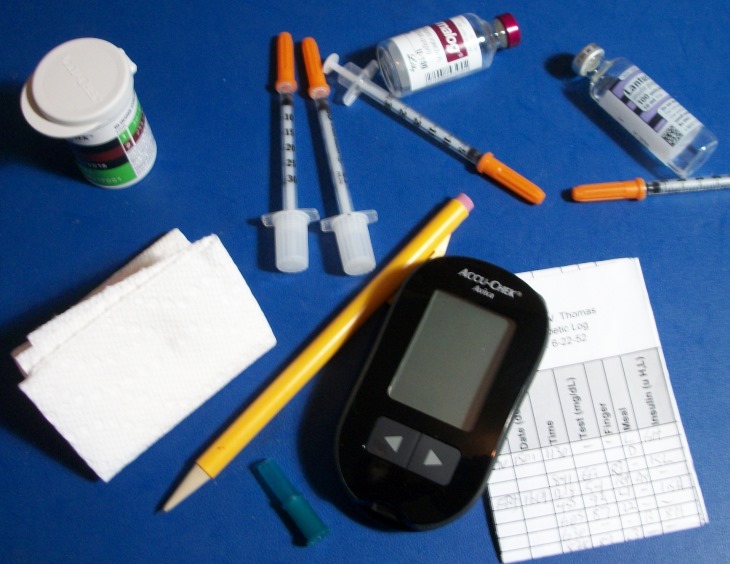
Below is a bulleted description of the method I use to safely maintain normal, non-diabetic blood-sugars:
- Blood-sugar is always either rising or falling. It is never static. My control method is to independently control both directions. Insulin is the downward (coarse) control element and “snacks” are the upward (fine) control element. Insulin is the coarse element because it is slower than the snacks. It is adjusted to maintain a continuous downward blood-sugar bias. The “snacks” are quick making upward adjustments with fine resolution.
- Note: The snacks are for control, not recreation!
- The control goal is to dither blood-sugar between 70 mg/dl and 100 mg/dl with 80 mg/dl as the target.
- I use syringes instead of an insulin pump to maximize manual control.
- Due to the nature of a Whole Foods Plant Based Starch centered diet and this method of control, my blood insulin level is routinely below “normal” on blood-work tests. This means this diet and control method results in a very high metabolic efficiency.
- I employ double blood-sugar tests, 15 minutes apart to determine rise or fall rate to predict when blood-sugar will drop below 70 or rise above 90.
- An appropriate snack is used when the double test predicts when blood-sugar will cross the 70 mg/dl threshold. Example; if the first test is 88 mg/dl and the second test is 80 mg/dl, then the fall rate is about ½ mg/dl per minute (8 mg/dl difference/15 minutes). With that, it can be predicted that the 70 mg/dl limit will be reached in 20 minutes (10 mg/dl difference / 0.5 minutes). A 20 minute snack should then be selected.
- Snacks are 60 to 80 calories per dose. Apple juice is the fastest; responding in about 5 minutes, a banana or medjool date is about 20 minutes, an apple is about 25 minutes and very mild. A fat-free starch (one ounce of rice, potato, rice cake, etc.) is about 20-30 minutes with several hours hold time. Needing a juice means late or insufficient testing and obviously should be avoided. While the reaction rate of juice can offer excellent, flat blood-sugar control, it is very poor in nutrients and worse; elevates your triglycerides.
- All snacks must have less than 10% fat. More than 10% fat adds insulin resistance dulling control and energy. Never, ever use comercial candy for a snack! Not only is the response poor and unpredictable, it induces insulin resistance, blowing tight control for over two weeks. I keep a stash of snacks in my car, pockets, back-pack, at work, etc. I make sure I am never without.
- If the 15 minute test indicates that blood-sugar will rise over 100 mg/dl an hour or more before the next meal, I will take one or two units of Humalog depending on the rise rate. I will allow it to reach as high as 130 mg/dl, if it peaks with a meal and the duration is less than an hour, but is strongly avoided. I don’t like the way I feel with blood-sugar ramping over 100 mg/dl and I fear it is damaging. The adjustment insulin rate is determined from the log. This is harder to figure out, because of all the variables and slower rate, which is a primary reason for taking insulin for a continuous downward blood-sugar bias and fine tuning with snacks.
- Each meal’s insulin is always taken five to fifteen minutes before a meal. The timing is determined from the logs recent history and learned blood-sugar response rate of the particular meal. The goal is to match the insulin action peak to the meal’s glucose conversion peak for a flat blood-sugar result plus enough for a downward ramp after the flattened glucose conversion peak.
With direct control of both directions of blood-sugar migration using double testing, preemptive insulin injections for continuous downward blood-sugar bias, fine-tuned with snacks, it is possible to maintain flatter blood-sugar levels than a normal, health non-diabetic because the non-diabetic’s blood-sugar is always controlled after-the-fact. That is; blood-sugar has to rise before the pancreas can respond.
The description of this method may seem hard, busy and consuming, however once you get used to it, it feels perfectly natural. And, I enjoy all the snacks throught the day! Over all these years, the Type-1 diabetes and my control method has never been a restriction on my life - indeed, it has been an enhancement! I feel that if I am going to have a “dreaded disease”, I might as well use it to my advantage!
IMPORTANT: please see my disclaimer.
DrCarney.com allows Member Blogs. Opinions in Member Blogs are views of the Member Blogger and not necessarily of Dr. Carney. Registered Users may request a FREE upgrade for blogging permission. Bloggers agree to support Dr. Carney's Starch-Smart-System.
When you subscribe to the blog, we will send you an e-mail when there are new updates on the site so you wouldn't miss them.


